


1Centre for Population Health Sciences (CePHaS), Lee Kong Chian School of Medicine, Nanyang Technological University, Clinical Sciences Building, 11 Mandalay Road, Singapore, Singapore, 2Queensland University of Technology, Kelvin Grove, Queensland, Australia, 3Research Institute for Primary Care and Health Sciences, Keele University, Staffordshire, UK, 4Dermatology Service, KK Women’s and Children’s Hospital, Singapore, 5National Skin Centre, 1 Mandalay Road, Singapore, and 6Global eHealth Unit, Department of Primary Care and Public Health, School of Public Health, Imperial College London, London, UK
#Both authors contributed equally to this manuscript.
This study examined concordance between caregiver-reported and physician-rated estimates of severity of atopic dermatitis (AD) in paediatric patients and explored potential explanatory factors. Physician-reported severity of AD was retrieved from medical records, while caregiver-reported disease severity and sociodemographic data were obtained through a survey that also collected information on out-of-pocket expenses due to AD. There was 38.5% (95% confidence interval (95% CI) 30.1, 43.5) disagreement between physician and caregivers with regards to both underestimating and overestimating the condition. A duration since AD diagnosis shorter than 6 months showed higher concordance (kappa: 44.4%; 95% CI 30.6, 58.2) between caregiver and physician estimates of AD severity compared with a duration of 6 months or longer. Caregivers underestimating their child’s AD accounted for 27.7% among all participants, while 10.8% overestimated the severity of AD compared with physicians. Factors significantly associated with caregiver’s underestimation of disease severity were age of the child and time since disease diagnosis. Comparison of concordance between caregiver-reported and physician-rated estimates of severity of AD in paediatric patients revealed a tendency amongst caregivers to underestimate severity of AD. This information may have clinical implications for treatment outcomes if caregivers fail to adhere to medical advice.
Key words: dermatitis; atopic; quality of life.
Accepted May 26, 2020; Epub ahead of print Jun 3, 2020
Acta Derm Venereol 2020; 100: adv00308.
doi: 10.2340/00015555-3540
Corr: Josip Car, Centre for Population Health Sciences (CePHaS), Lee Kong Chian School of Medicine, Nanyang Technological University, Clinical Sciences Building, 11 Mandalay Road, Singapore 308232, Singapore. E-mail: josip.car@ntu.edu.sg
This study reveals discordance between caregiver-reported and physician-rated severity of childhood atopic dermatitis (AD). Physicians and parents value different aspect in assessing severity of AD. This study examined the measures from a real-life perspective. The results also show that caregivers may have a better understanding of severity, given that they see the child on a daily basis. Physicians should therefore work in partnership with caregivers to encourage adherence to treatments. This information sheds light on when parental understanding of severity is differently understood, which is an important step in improving adherence to treatment recommendations.
Atopic dermatitis (AD) is a common chronic dermatosis characterized by flare-ups of red itchy skin, that affects both children and adults (1). The condition can have a profound impact on both patients’ and caregiver’s health-related quality of life (HRQoL) and can often affect the whole family. Suboptimal control of AD can result in adverse outcomes, such as severe itching, sleep disturbance, mood changes and psychosocial impairment (2, 3). The severity of the disease often predicts health status, with more severe AD associated with lower HRQoL (4).
Although AD is highly prevalent in children worldwide, little is known about how caregivers’ and physicians’ estimated severity of the condition are in alignment (5). Estimating the severity of AD is an important step in understanding the level of ill-health and establishing the baseline level, which can be used to plan appropriate disease management, including alleviation of any accompanying burdens (6). Several scoring systems for severity of AD exist (Eczema Area and Severity Index (EASI), Investigator’s Global Assessment scale, Scoring Atopic Dermatitis) and they generally rely on health professionals’ medical expertise and knowledge of assessing the intensity of signs and symptoms (7–9). However, this clinical opinion may differ substantially from patients’ and caregivers’ subjective assessment of the severity of AD (7). Caregivers often assess the degree of severity of their child’s condition based on their own subjective feelings and observations, and often include symptoms not included in the physician’s assessment, e.g. emotional burdens (10, 11). Caregivers see the child on a daily basis, while the physician often makes an assessment based on one visit or more. It is not uncommon that physicians and parents have different views of the child’s AD, a divergence that potentially could affect caregivers’ approach to treatment and disease management (12). This could subsequently lead to negative health outcomes, e.g. lower adherence to following physicians’ recommendations. There is therefore a need to assess how the views of caregivers and physicians may differ and to identify associated factors, so that measures can be taken to improve the mutual understanding of the severity of the child’s AD. This is of importance, as the caregiver and physician must form a partnership where the latter educates the former to enable self-management, with the mutual goal of optimizing care for the child (7). A previous study from primary care found that AD is often described by physicians in a medical physical way, whereas caregivers emphasize the psychosocial impact and emotional wellbeing (12).
Hence disease perception may play a significant role when caregivers monitor and make treatment decisions regarding the child’s AD on a daily basis in improving the condition and subsequently also HRQoL (7). Exploring discrepancies between physicians and caregivers regarding their severity level estimation of AD can shed light on when severity is differently understood and provide information that can be used to improve parental adherence to treatment recommendations (13, 14). This study therefore aims to explore the concordance between caregiver-reported and physician-rated severity of AD in paediatric patients as well as to investigate potential explanatory factors.
Design and participants
A cross-sectional study was conducted between December 2016 and December 2017 at 2 paediatric dermatology clinics in Singapore. Eligible participants were referred to the study team by the treating physician. Patients and caregivers were eligible for participation if they were below 16 years of age, fulfilled the Hanifin and Rajka criteria for AD (8), understood English and/or Mandarin, and if the caregiver was the legally authorized representative (LAR) for the child.
Covariables
Patients and caregivers completed a questionnaire that included background information, such as sociodemographic data, as well as questions about weekly out-of-pocket expenses related to the child’s AD for purchases of non-medical products and services, e.g. over-the-counter moisturizers, laundry services, and special diet food. Those costs were attributed to the cost year of 2017 and assumed the annual cost per child. The questionnaire also obtained caregiver reported time spent on informal caregiving (h per week) due to the child’s condition. Informal caregiving comprised care that parents provided in caring for the child’s AD based on pre-set activities: personal care, preparing special meals because of dietary restrictions, and providing emotional support (15). Child’s age was grouped into 3 ranges (less than 2 years old, 2–4 years old and 4–16 years old) as suggested by dermatology experts (dermatologists in participating paediatric dermatology clinics) reflecting the major stages of child development (16).
Severity assessment
During the clinic, dermatologists recorded disease conditions in the medical notes (physician-rated disease severity), assessed whether the patient was eligible for the study, and referred suitable patients to the research team. The research team then approached them and asked the caregivers to complete the questionnaire and assess the severity of their child’s AD (caregivers perceived disease severity).
Caregivers perceived disease severity was collected when they visited the dermatology clinic. They were required to report whether they perceived their child’s AD severity as mild, moderate or severe. They were advised to answer this question based on how they perceived their child’s current condition rather than their overall impression of the disease.
Physician-rated disease severity was based on information recorded in the electronic medical records (EMR) on the same day as caregivers visited the dermatology clinic and rated the current severity of their child’s AD. At both study settings, physicians applied a modified Physician Global Assessment (PGA) when rating the severity of AD (8): Clear refers to “no inflammatory signs of atopic dermatitis”’; Almost clear refers to “faint, barely detectable erythema and/or trace residual induration/papulation in limited areas; neither excoriation nor oozing/crusting are present”; Mild refers to “light pink erythema and slightly perceptible induration/papulation; excoriation are present”; Moderate refers to “’dull red, clearly distinguishable erythema and clearly perceptible induration/papulation but not extensive; excoriation or oozing/crusting are present”; Severe refers to “deep/dark red erythema, and marked and extensive induration/papulation; excoriation and oozing/crusting are present”. For those patients whose severity was not explicitly reported in the electronic medical records, symptoms and affected area were extracted and classified by an investigating physician-researcher (XM), who had received training in dermatology and EASI scoring, using EASI calculator, into mild (EASI score 1.1–7.0), moderate (EASI score 7.1–21.0), severe (EASI score 21.1–50.0), and very severe (EASI score 50.1–72). This score is calculated by estimating the percentage of skin affected and the extent of redness, thickness, scratching, and lichenification, respectively, at 4 body sites (17).
Statistical methods
According to the sample size formula for a quantitative variable, the minimum sample size required was estimated by assuming a 20% prevalence of AD among children (age ≤18 years) in Singapore (18, 19). Furthermore, we also considered a type-1 error rate of 5%, 80% power, a 5% permissible margin of absolute error, and a 10% non-response rate. Using the 1-proportion hypothesis testing formula, the minimum required sample size was calculated to be 518 patients. Descriptive statistics were performed, using median with interquartile range (IQR) for continuous variables and frequencies and percentages (%) for categorical variables. We assessed agreement between physician-rated severity and caregiver perceived severity with Cohen’s kappa (14). The kappa statistics was interpreted as “slight agreement” (0.01–0.20), “fair agreement” (0.21–0.39), “moderate agreement” (0.40–0.60), “substantial agreement” (0.61–0.80) and “almost perfect agreement” (0.81–1.00) (15). Multivariable logistic regression analyses were performed to estimate factors associated with both the underestimation and overestimation of the severity of the condition in relation to the physicians rating. Odds ratios (OR) were calculated for each variable and reported with 95% confidence intervals (95% CIs). Clinically meaningful interactions were checked and considered significant if p < 0.1. We checked for multicollinearity between covariates using collinearity diagnostics. Variables with a condition index of ≥ 30% or a variance-decomposition proportion of ≥ 50% were considered to be causing collinearity problems (20, 21). All statistical analyses were undertaken by using Stata version 14.2 (StataCorp, College Station, TX, USA). Two-sided p-value less than 0.05 was considered statistically significant.
Ethics approval
This study was carried out in accordance with the recommendations in the NTU-IRB Guidelines. Ethical approvals were obtained from the Institutional Review Board of National Healthcare Group (NHG-DSRB: 2015/01228) and Nanyang Technological University (NTU IRB: IRB-2016-10-059-01).
Social demographic and baseline data
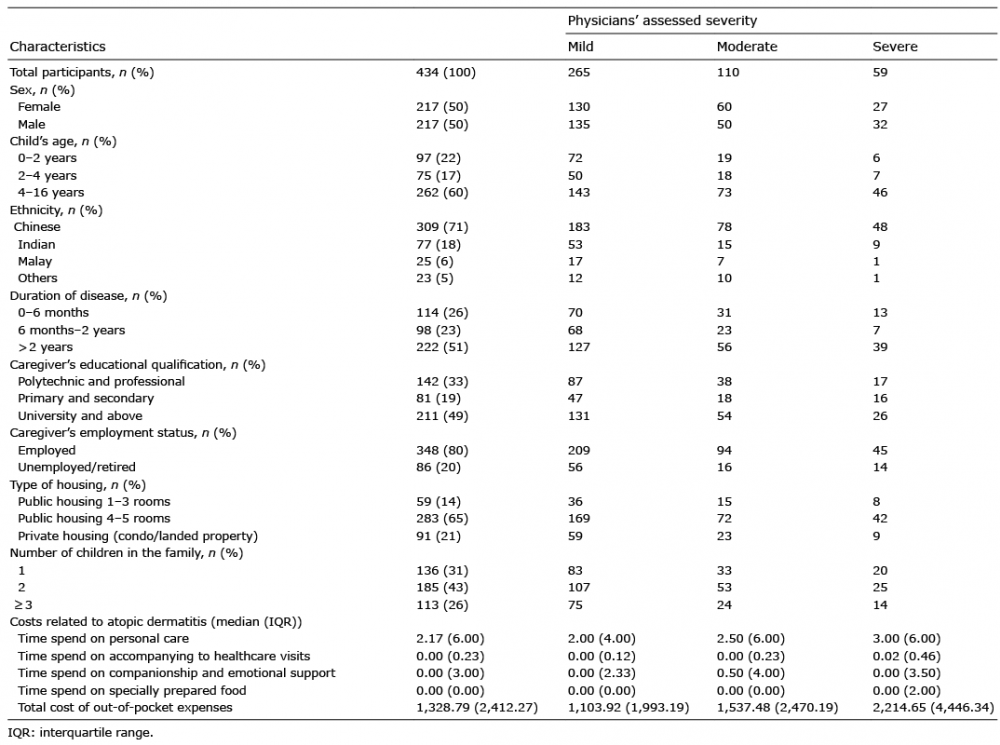
The characteristics of the participants are summarized in Table I. A total of 434 patients with an equal sex distribution were included in the study (559 participants were recruited for the study, among which, 125 were excluded due to missing information). Of the sample, 22% of the children were 0–2 years of age, 17% were 2–4 years of age, and 60% were 4–16 years of age. The majority of participants were Chinese (71%). Caregivers with professional degrees or university educations accounted for 81% of the sample. The most common housing type was government flats (public housing 1–3 rooms: 17%; public housing 4–5 rooms: 65%). With regards to family size, 31% of families had one child, 43% had 2 children and 26% had more than 2 children.
Table I. Study participants and their caregiver’s characteristics regarding severity of atopic dermatitis
Agreement of severity rating
Overall concordance between caregiver-perceived and physician-rated severity of AD was 62%, while 28% and 11% of caregivers underestimated and overestimated severity compared with physicians’ ratings. Crude agreement and kappa statistics for concordance and discordance are displayed in Table II. Type of housing is an indicator of socioeconomic status in Singapore; the current study showed that participants living in smaller government flats had the lowest concordance (kappa statistic 27%). With regards to the duration of disease, there was a fair agreement in AD severity grading between caregivers and physicians if their child’s duration was between 6 months and 2 years (kappa statistic 37%) or more than 2 years (kappa statistic 33%). Fair agreement was found in children older than 2 years of age (2–4 years old: kappa statistic 30%; 4–16 years old: kappa statistic 35%). For employment status of caregivers, those that were currently employed had higher concordance than unemployed or retired caregivers (employed caregivers: kappa 38.1%; unemployed/retired: kappa 31%). With regards to family size, there was higher concordance in families with one child (kappa 40%) and a similar trend was detected for lower concordance for families with more children (2 children kappa 36%; >3 children kappa 35%).
Table II. Concordance and discordance in physician and caregiver rated severity of the child’s atopic dermatitis
Multivariable regression analyses
The multivariable regression analyses for caregivers who underestimate children’s disease severity compared with physicians’ assessment can be seen in Table III. Through our multivariate analyses models it was found that caregivers to children between 4 and 16 years of age (OR: 5.50, 95% CI: 1.36, 22.21, p = 0.017) and caregivers to children between 2 and 4 years of age (OR: 4.20, 95% CI: 0.92, 19.08, p = 0.063) might also influence the underestimation of the disease severity. Also, children with a disease duration of 6 months to 2 years (OR: 0.24, 95% CI: 0.06, 0.94, p = 0.04) were more likely to underestimate their child’s disease severity. Another statistically significant factor associated with caregivers underestimating their child’s AD severity was disease-related out-of-pocket expenses per 1,000 US$ (e.g. moisturizing creams, special hygiene products, additional costs for laundry, etc.) (OR: 1.05, 95% CI: 1.01, 1.09, p = 0.011). Approximately 14.7% of the caregivers who underestimated their child’s severity also had out-of-pocket expenses ≥ US$10,000 per year (95% CI: 10.2, 19.2). Sociodemographic characteristics (sex, ethnicity, educational attainment, caregiver’s employment status, number of children in the family and type of housing) did not reveal any significance in the model. Model discrimination (c-statistics) was employed to test overall goodness-of-fit for the logistic model was 0.785 and calibration (Hosmer-Lemeshow test p-value) was 0.642. No significant associations were found for any factors when tested for overestimating AD severity (see Table SI). Overall goodness-of-fit for the logistic model was 0.6002 and calibration (Hosmer-Lemeshow test p-value) was 0.248.
Table III. Multivariable logistic regression analysis of factors associated with underestimation of the severity of atopic dermatitis (AD)
Our findings revealed an overall discordance of 39% between caregiver-perceived severity of AD and physician-rated severity. There was also a trend that discordance increased when AD was more severe. Caregivers tended to rate their child’s AD severity lower than did the physician (28%). This finding is in alignment with a previous study, which assessed patient self-reported and physician-rated AD severity in adults and estimated a 31.4% discordance where patients rated their disease severity lower than physicians (22). Knowing that as much as 28% of caregivers underestimate their child’s AD severity may have important clinical implications for treatment adherence.
Caregivers play a key role in managing their child’s AD, and if parents underestimate the severity of their child’s AD, it may lead to under-treatment of the condition, e.g. neglecting to apply topical steroids, emollients and follow dietary restrictions (23, 24). There is also a risk that some caregivers may resort to complementary and alternative medicine for their child’s AD, without involving a physician (23). This poses risks, as the clinical effectiveness of these interventions is often unclear and complementary treatments may have adverse effects when used alone or in combination with pharmacological agents (25).
This can lead to a undesirable consequences, e.g. use of unregulated medications, if caregivers are unable to differentiate between various degrees of severity and symptoms thereof, and do not properly know how and when to medicate or consult healthcare professionals (24). Another aspect commonly associated with poor treatment outcomes in AD patients is the suboptimal use of topical corticosteroids. One study showed that as much as 20% of caregivers did not use topical steroids even during severe disease (26). Therefore, a consensus of level of severity between caregivers and physicians is extremely important, as AD, being a chronic disease, requires self-involvement in severity recognition and adherence to physician-recommended treatments, to achieve better treatment outcomes (27). Both the physician’s severity rating and caregiver’s assessments are also required to guide future therapeutic decisions and treatment pathways. It should, however, be noted that caregivers underestimating AD severity is not the only reason for suboptimal use of therapy and that there may be other contributing factors, such as steroid phobia amongst parents, as well as cost of medication and other reasons (28, 29).
Although underestimation of severity may be associated with adverse AD outcomes, it could also be a positive aspect if overtreatment is avoided, as the physician may not always know best. For example was it reported in a German study that oral systemic steroids were prescribed to 10% of the children in a study sample, whereas the proportion of ones that actually needed it was likely to be much lower (30).
Our findings show that discordance was associated with older age of the child (age 4–16 years of age) as well as a moderate time since AD diagnosis of 6 months to 2 years. We speculate that this could potentially be associated with increased habituation to a chronic condition over time, or that AD may appear subjectively worse in infants compared with older children (since it may cover more skin area, the child may cry more, etc.). Another possible explanation is that older children with AD may manage their treatment with less caregiver involvement; hence the parent is not as aware of the condition status (for older children). As the management of AD relies upon appropriate disease monitoring, it is important to identify factors associated with severity rating discordance between caregivers and physicians (31).
For the finding that concordance between caregivers and physicians was better for children with AD with a short time since diagnosis, a previous study assessed caregiver-estimated AD severity, compared with the physician-rated severity, and found similarities between physician and parent assessed severity, which decreased after a visit to physician specialist (32). A possible explanation for this could be that the caregivers’ perception of the degree of seriousness and individual attachment to AD includes expectations about scope and duration of symptoms, which are not fixed ideas, and changes over time as knowledge, treatment options and the level of fear and threat changes (33). Hence, initial perceptions of severity of AD may lower as the understanding of available treatments and symptomatic control gives caregivers a sense of control over the disease and they regard it as less of a threat to the child’s health.
Caregivers’ health knowledge may also play a significant role in their perception of the severity of AD, and this may have a substantial impact, not only on providing adequate medical history but also on adherence to physician recommended treatments (7). Low caregiver health literacy and poor knowledge about AD severity can lead to increased stress in caregivers, possibly generating poorer perceived health status and lower HRQoL for the child and family (34, 35).
An unexpected finding of this study was the association between caregiver underestimation of AD and increased out-of-pocket expenses, which cannot be explained by this study, as the analysis did not include testing for casualties. It could, however, be argued that parents not perceiving their child’s condition as severe are more prone to self-treat with over-the-counter (OTC) alternatives. As seen in one study in which caregivers bought OTCs, such as non-medical moisturizers, coconut oil and herbal remedies, believing that they would cure, be sufficient management for AD or a “safer” alternative to medical drugs (12).
Limitations
Limitations of this study include several sources of potential bias and imprecision, since all study subjects were recruited from specialized healthcare settings. Since participants were only recruited from tertiary hospitals, they might have been experiencing more severe disease conditions compared with those who visited primary care clinics. However, this limitation could be compensated, to some extent, because of the particularity of paediatric diseases: parents have a tendency to turn towards tertiary care instead of visiting primary hospitals (e.g. visiting their GP) as they think paediatricians are generally better trained and equipped to diagnose diseases in children. As such, the major hospitals in this study cover the larger proportion of paediatric patients. Besides selection bias, other systematic error could have affected the results, for example omitted variable bias, since our regression models omitted variables not relevant for this study as it was part of a larger project. Furthermore, other explanatory factors not captured in the questionnaire could have affected the discordance between the caregiver and physician estimates of disease severity in AD. We also acknowledge that using different tools for physicians and caregivers is somewhat problematic, since a proper comparison cannot be made. One assessment comes with detailed instructions and may vary among different physicians, whilst the other is based on subjective perception. However, as previously reported, physicians and parents’ perspectives are different and they value different aspects when making severity judgements: physicians are likely to rely on evaluating visual signs, supplemented by a brief history, while caregivers are prone to evaluate symptoms/complaints from their child’s behavior as well as observed visual signs. Hence this study captured the measures from a real-life perspective (12). It is not unlikely that caregivers may have a better understanding of severity, and that physicians might overestimate AD. Therefore physicians should take caregiver’s perceived disease severity into consideration, in order to assist them in making a more precise clinical decision. Social context may also play a role by influencing the understanding of the terms mild, moderate and severe degrees of AD; based on what other hardships the family may face, itching may not be a great concern.
Conclusion
Discordance between physicians’ rating and caregivers’ perception of disease severity for paediatric AD shows a tendency amongst caregivers to underestimate the disease severity. This information may have clinical implications for treatment outcomes if caregivers fail to/avoid adherence to medical advice. Future research in this area should include more potentially explanatory variables and study larger sample sizes in order to generate more robust findings.
The authors would like to thank all children and caregivers that responded to the questionnaire and made this study possible.
This research was supported through the Skin Research Grant by the Skin Research Institute of Singapore (SRIS), a tripartite partnership between the Agency for Science, Technology, and Research (A*STAR), National Healthcare Group through its National Skin Centre (NHG) and the Nanyang Technological University (NTU).
Informed consent was obtained from all individual participants included in the study. Written informed consent was obtained from the legally authorized representative (LAR) of the child prior to enrolment in the study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize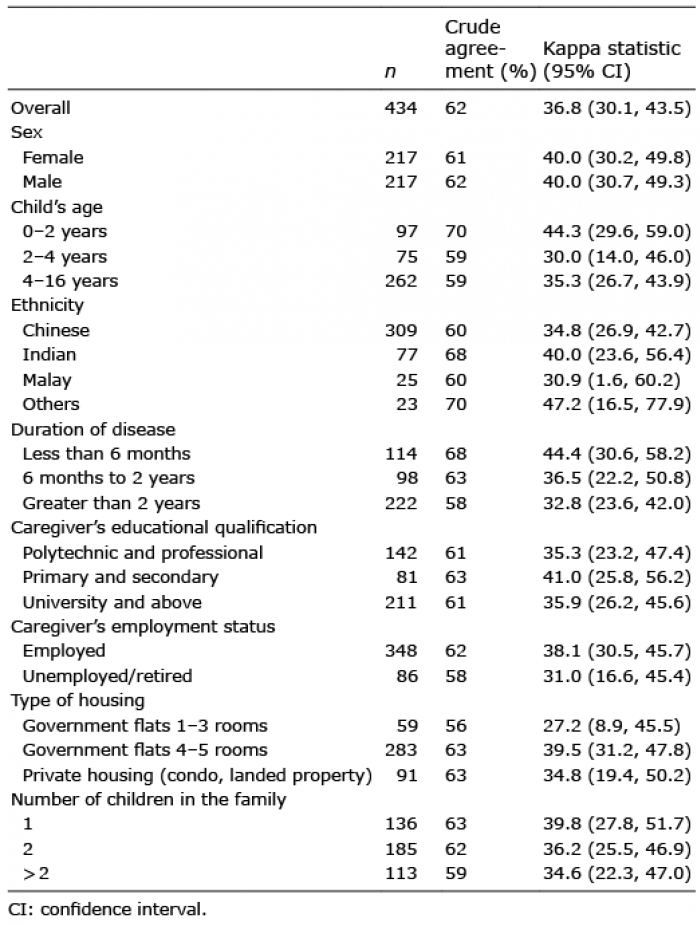 Click to show fullsize
Click to show fullsize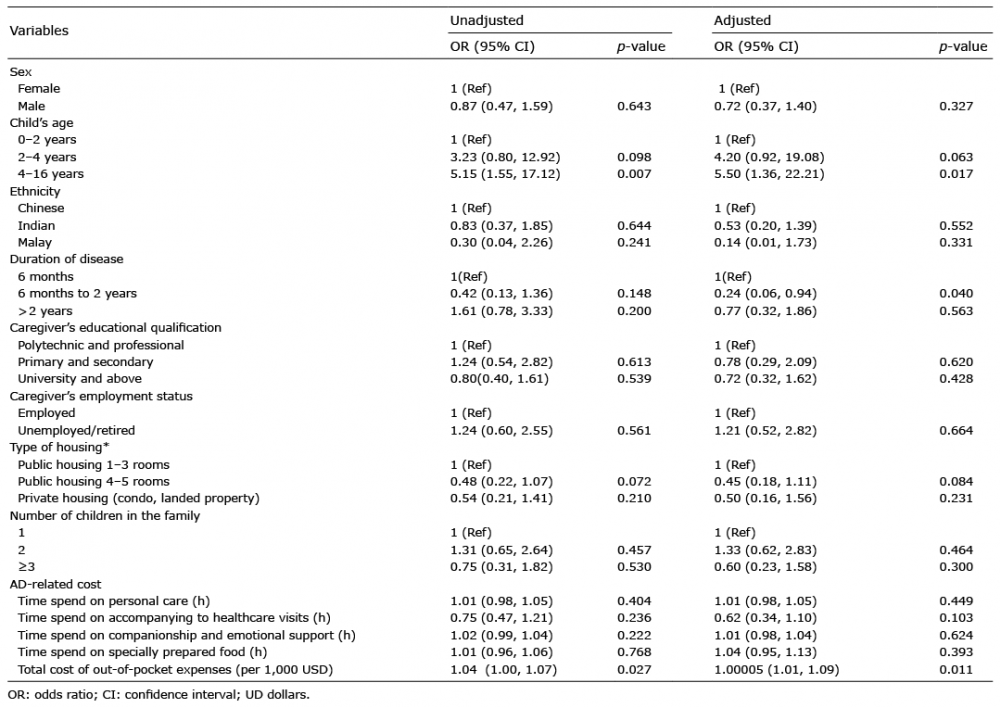 Click to show fullsize
Click to show fullsize